Top 15 Compliance Failures in DDD, Assisted Living & Behavioral Health Homes
Here’s the uncomfortable truth most owners don’t hear until the exit conference:
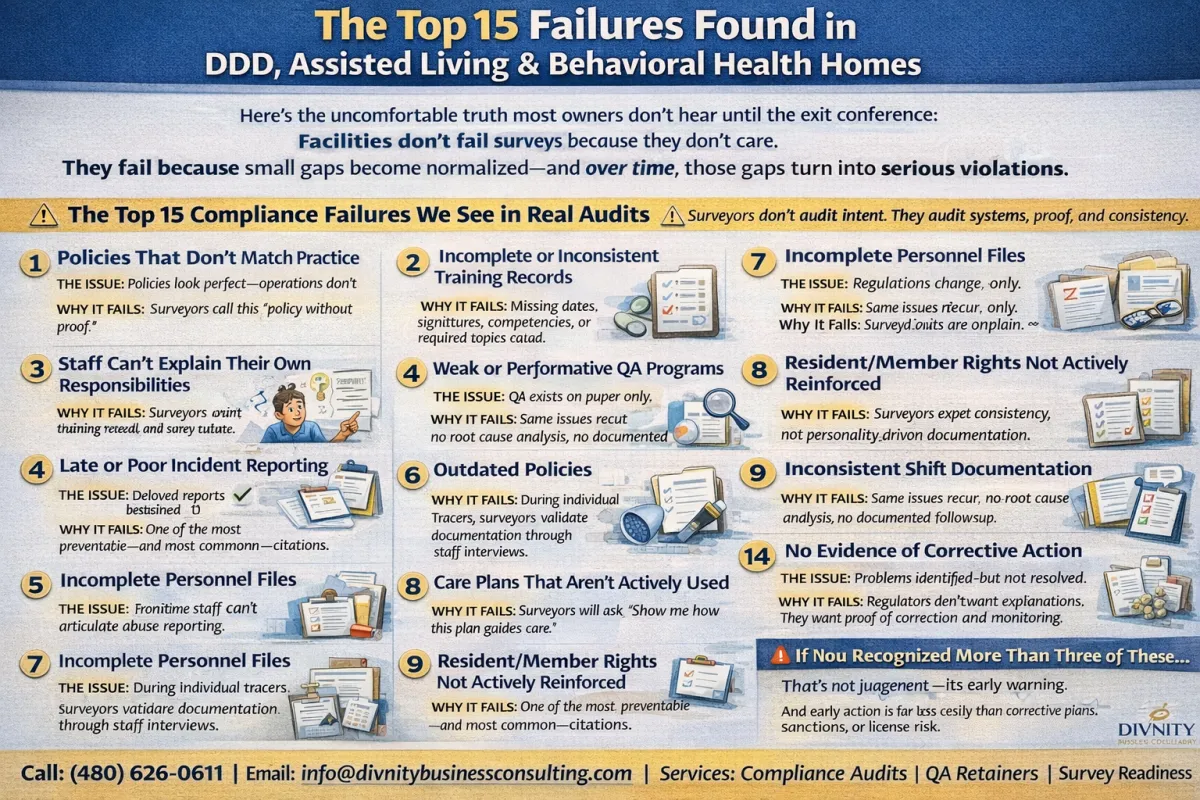
Facilities don’t fail surveys because they don’t care.
They fail because small gaps become normalized—and over time, those gaps turn into serious violations.
Across DDD group homes, Assisted Living, and Behavioral Health facilities, the same compliance failures appear repeatedly. As 2025 audit trends show, surveyors are assigning higher severity to systemic breakdowns, not just isolated mistakes.
If you’ve been cited before—or want to avoid your first major deficiency—this list matters.
The Top 15 Compliance Failures We See in Real Audits
⚠️ Surveyors don’t audit intent. They audit systems, proof, and consistency.
1. Policies That Don’t Match Practice
The Issue: Policies look perfect—operations don’t.
Why It Fails: Surveyors call this “policy without proof.”
If daily practice doesn’t align with written policy, it signals a breakdown in operational discipline and safety culture.
2. Incomplete or Inconsistent Training Records
The Issue: Training happened. Documentation didn’t.
Why It Fails: Missing dates, signatures, competencies, or required topics equal noncompliance.
Training must show attendance, comprehension, and competency, not just intent.
3. Staff Can’t Explain Their Own Responsibilities
The Issue: Frontline staff can’t articulate abuse reporting, incident response, or resident rights.
Why It Fails: During Individual Tracers, surveyors validate documentation through staff interviews.
If staff can’t explain their role, it’s a system failure, not an employee issue.
4. Weak or Performative QA Programs
The Issue: QA exists on paper only.
Why It Fails: Same issues recur, no root cause analysis, no documented follow-up.
Surveyors spot patterns faster than leadership does when QA lacks teeth.
5. Late or Poor Incident Reporting
The Issue: Delayed reports, incomplete narratives, missing corrective actions.
Why It Fails: This escalates quickly—especially in DDD and Behavioral Health.
Incomplete reporting raises immediate safety and oversight concerns.
6. Outdated Policies
The Issue: Regulations change. Manuals don’t.
Why It Fails: Surveyors expect policies to reflect current law, not last year’s template.
Outdated policies are one of the easiest—and most avoidable—citations.
7. Incomplete Personnel Files
The Issue: Missing background checks, credentials, job descriptions, or evaluations.
Why It Fails: Personnel files are compliance landmines.
Surveyors rely heavily on these to verify competence and supervision systems.
8. Care Plans That Aren’t Actively Used
The Issue: Care plans exist, but staff don’t reference them.
Why It Fails: Surveyors will ask, “Show me how this plan guides care.”
If staff can’t demonstrate use, the plan is considered ineffective.
9. Medication Documentation Gaps
The Issue: Meds administered correctly—documentation isn’t.
Why It Fails: Missing signatures, incorrect times, no variance explanations still count as violations.
The MAR must be completed immediately after administration. No exceptions.
10. No Proof of Supervision
The Issue: Supervision is claimed, not evidenced.
Why It Fails: If it’s not documented, it didn’t happen.
Surveyors cross-check supervision levels against incidents, falls, and assessed risk.
11. Emergency Preparedness Is Theoretical
The Issue: Plans look good. Staff don’t know them.
Why It Fails: Surveyors want training records and drills, not binders on shelves.
Knowledge and execution matter more than formatting.
12. Resident/Member Rights Not Actively Reinforced
The Issue: Rights posted ✔️ Explained ✖️ Acknowledged ✖️
Why It Fails: One of the most preventable—and most common—citations.
Surveyors will ask residents directly what they understand about their rights.
13. Inconsistent Shift Documentation
The Issue: Each staff member charts differently.
Why It Fails: Surveyors expect consistency, not personality-driven documentation.
Inconsistency undermines continuity of care.
14. No Evidence of Corrective Action
The Issue: Problems identified—but not resolved.
Why It Fails: Regulators don’t want explanations. They want proof of correction and monitoring.
15. Leadership Too Far Removed From Operations
The Issue: Leadership oversight is distant or passive.
Why It Fails: Surveyors evaluate leadership’s role in sustaining a culture of safety.
Without visible, active leadership engagement, compliance erodes quietly.
Why These Failures Keep Happening
Most facilities rely on:
Templates without customization
One-time audits instead of systems
Compliance “check-ins” instead of active oversight
Compliance isn’t an event. It’s a discipline.
How DiVnity Business Consulting Fixes This
We don’t just identify failures—we eliminate repeat citations by:
✔ Aligning policy with real workflows
✔ Building staff-ready documentation systems
✔ Installing QA structures that self-correct
✔ Training leadership to think like regulators
That’s how facilities stop cycling through the same deficiencies.
🚨 If You Recognized More Than Three of These…
That’s not judgment—it’s early warning.
And early action is far less costly than corrective plans, sanctions, or license risk.
📞 (480) 626-0611
📧 [email protected]
📋 Services: Compliance Audits | QA Retainers | Survey Readiness
